Bacteria Eaters: The “Twort-d’Hérelle Phenomenon”
by John Emrich and Charles Richter
December 2021
Two decades after diphtheria antitoxin became a clinical success at the end of the 19th century, greatly reducing death from the disease, especially among young children, a new phenomenon with claims of vast therapeutic potential against bacterial infections burst onto the scene. The “Twort-d’Hérelle Phenomenon,” also known as “transmissible lysis of bacteria,” was named after its two co-discoverers: Frederick William Twort and Félix Hubert d’Hérelle. We know it now as bacteriophage.
The Discoveries of Bacteriophage
 Frederick Twort, c. 1914
Frederick Twort, c. 1914
Biogr. Mem. Fellows R. Soc.In 1915 Twort, a British physician and microbiologist, published a paper in the Lancet describing a “glassy and transparent” transformation on agar plates where bacteria would not grow even when subcultured. He was able to take samples from the glassy area of the colony and replicate results over multiple generations of micrococcus, demonstrating that the agent was transmissible. These samples remained lethal to bacterial cultures even after passing through a fine porcelain filter that would trap bacteria. Further, Twort concluded that the substance required bacteria for growth. He postulated that the micrococcus itself might be secreting an enzyme able to pass through a filter that both caused lysis and stimulated further enzyme production, and that this transmission “might almost be considered as an acute infectious disease of micrococci.” Before Twort could conduct further experiments, however, the First World War interrupted his career. As the paper was about to go to press, he joined the Royal Army Medical Corps and was shipped out to Greece. Following the war, Twort moved “on to other work.”
In 1917, independent of Twort’s research, d’Hérelle, a French-Canadian microbiologist researching enteric bacteria of dysentery patients at the Pasteur Institute, published a short paper in Comptes rendus de l’Académie des Sciences describing the lysing of bacteria over multiple propagations. He named this “invisible microbe that is antagonistic to the dysentery bacillus” the bacteriophage (a bacteria-eater, from the Greek phagein meaning "to devour"). D’Hérelle concluded his paper with a few observations: that the bacteriophage is a “microbe of immunity;” it has specificity; and there is a real potential to treat bacterial infections with phage therapy.
D’Hérelle would publish a few more short bacteriophage papers in Comptes rendus before publishing his first book Le Bactériophage: son rôle dans l’immunité (The Bacteriophage: Its Role in Immunity) in 1921. It was this book, and the English translation by Yale University bacteriologist and immunologist George H. Smith (AAI 1918), published by Williams and Wilkins in 1922, that popularized bacteriophage therapy.
The Dominant Theories of Immunity
 Félix d’Hérelle
Félix d’Hérelle
Smithsonian ArchivesTo understand d’Hérelle’s use of the word “immunity” in his first paper and in the title of his book, it would help to first consider the competing theories of immunity at the time and how the bacteriophage aligned or conflicted with them.
In the late 19th and early 20th centuries, the term immunity was frequently used to describe resistance to “natural” infections, whereas immunity acquired through vaccination was considered something different. And for researchers at the time, “it was not at all clear that ‘natural’ immunity and ‘acquired’ immunity were mechanistically related.” Further, there were two divergent theories attempting to explain natural immunity: cellular, associated with Élie Metchnikoff; and humoral, associated with Paul Ehrlich.
Metchnikoff observed that when starfish larvae were punctured with a splinter, cells moved toward the injury and began to engulf foreign bodies. This led him to hypothesize that organisms had specialized cells that were able to defend against intruders. These cells that could identify, engulf, and kill foreign microorganisms were soon named “phagocytes.” In subsequent studies, Metchnikoff was able to observe that phagocytes have specificity as to which foreign organisms they attacked.
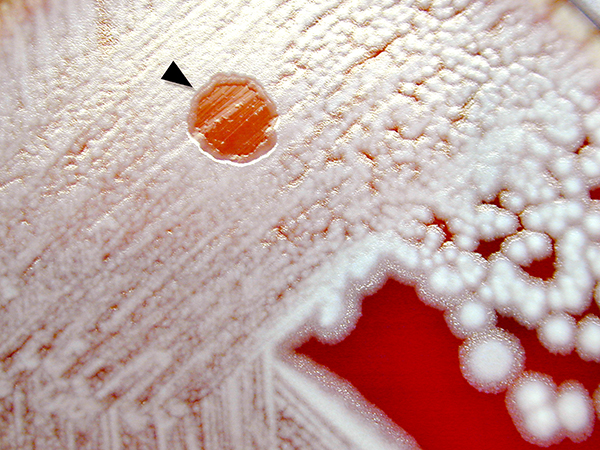 Petri dish showing phage-lysed bacteria culture
Petri dish showing phage-lysed bacteria culture
CDCEhrlich’s research about immunity was focused on how animals could acquire immunity against a disease through prior infection or vaccination—vaccines for smallpox and rabies were the only effective ones for humans at the time. It was known that human blood in in vitro experiments could agglutinate bacteria as well as a variety of “toxins,” like the one produced by diphtheria. To make sense of what was occurring in vivo, Ehrlich hypothesized, using chemistry terminology, that there were substances (perhaps proteins) in the blood that could act on a specific bacteria or toxin resulting in either “agglutination” (bacteria or other microscopic objects) or “flocculation” (toxins and soluble other substances). He later expanded this theory, once again using chemistry terminology, to try to describe the specificity of the agglutination and flocculation reactions. His addendum that the blood substances were composed of “core” and “side-chains” found some adherents, but subsequent research proved that the complexity of immune cells and substances could not be analogized easily to chemistry concepts.
 Élie Metchnikoff, 1913
Élie Metchnikoff, 1913
Gallica Digital LibraryFor their theories on the immune system, Metchnikoff and Ehrlich shared the Nobel Prize in Physiology or Medicine in 1908 “in recognition of their work on immunity.” Though both had adherents, in the late 19th century Ehrlich’s humoral theory was put into clinical practice by Émile Roux and Emil von Behring, who created the first successful diphtheria antitoxins and pushed the limits of serum therapy, which was a method to passively immunize humans and animals against specific diseases. (See “Hero Horses in the Fight Against Disease,” AAI Newsletter October 2021, for more information.) The clinical success of the diphtheria antitoxin raised the stature of Ehrlich’s theory as well as the potential for successfully curing, or even providing acquired immunity, against other bacterial infections.
Bacteriophagy Theory
Félix d’D’Hérelle, however, found that neither the humoral nor cellular theory of immunity fit his experimental observations using bacteriophages as a curative treatment. In experiments with chickens and humans, d’Hérelle provided results that showed bacteriophage therapy (also called bacteriophagy) could be successful in cases where the specific bacteria were known and the corresponding bacteriophage was provided to the subject. As a result, he proposed a new theory for immunity based on the bacteriophage.
 Paul Ehrlich
Paul Ehrlich
NLMAccording to historian of science William Summers, d’Hérelle understood “that in natural immunity (as opposed to the ‘artifactual’ situation of experimentally induced infections), man and animals resisted and eventually recovered from disease because of the appearance of phages which destroyed the infecting bacteria.” The evidence d’Hérelle used to support this understanding came from a dysentery study where patients recovering from their infection after the administration of a bacteriophage suspension specific to the bacterium responsible for their infection showed a remarkable increase of the titer of phage in their stool.
A two-phase mechanism for immunity by bacteriophagy was described in more detail by d’Hérelle in The Bacteriophage. After the specific bacterium responsible for the infection was identified, a bacteriophage specific to that bacterium was put into a suspension, which was then administered to the patient. The first phase, “exogenous immunity,” lasted 24 to 48 hours and was marked by the presence of “bacteriophage protobes virulent to the pathogenic bacterium.” The second phase, “endogenous immunity,” could last up to 14 months and was a response to a “stimulus being provided by the products of bacterial dissolution as contained in the bacteriophage suspension.” During an epidemic, the exogenous phase is maintained because the near constant reinfections maintain the bacteriophages.
For d’Hérelle, the bacteriophage, not a cellular or humoral response, was responsible for immunity, and by 1926 he was certain that bacteriophagy could be used to successfully treat bacillary dysentery, staphylococcus infections, and, potentially, bubonic plague.
Jules Bordet
Jules Bordet (AAI 1960). In the interim between d’Hérelle’s first bacteriophage article and the publication of The Bacteriophage, Bordet was awarded the 1919 Nobel Prize in Physiology or Medicine “for his discoveries relating to immunity.” The director of the Pasteur Institute in Brussels, Bordet had spent decades researching and describing the lysis process in vitro and in vivo. These included the discovery of complement, the development of complement fixation tests, the identification of the bacterium that causes whooping cough, and advances in understanding the bacteriolytic and hemolytic effects in vivo.
 Jules Bordet
Jules Bordet
NLMLacking sufficient magnification to see the bacteriophage, researchers could only understand it by observing its effects, fueling intense debate about what exactly the bacteriophage was—a lysing enzyme (Bordet) or a “microbe of immunity,” perhaps a virus (d’Hérelle)—and how it fit into the competing theories of immunity. As strange as it may seem today, Bordet’s concept of the bacteriophage as a “self-perpetuating lytic enzyme” fit neatly into the humoral theory and serum therapy and carried the prestige of a recent Nobel laureate. It would remain the dominant theory until advances in electron microscope magnification in the late 1930s.
Proliferation of Bacteriophage
The controversy surrounding the bacteriophage did not prevent the proliferation of corresponding research and clinical therapies. The success of diphtheria antitoxin provided a lesson in combatting bacterial disease with a humoral-based serum therapy. The hope was that the new phenomenon would pave the way for additional serum therapies for other bacterial infections in humans and animals.
While the vast majority of the early research with bacteriophages occurred in Europe (most notably in Paris, Brussels, and London), American researchers began publishing on the topic by the early 1920s, even prior to the translation of The Bacteriophage.
The first American institution to take bacteriophage seriously as a research topic was the Department of Bacteriology at the University of Michigan, chaired by Frederick G. Novy (AAI 1920, president 1924–25). Novy, who received his first shipment of bacteriophages from d’Hérelle in 1921, collaborated on this research with younger investigators in his department, including Paul de Kruif (AAI 1921) and Philip Hadley (AAI 1927). Hadley would go on to make significant contributions to bacteriophage research in the 1920s and 1930s. De Kruif left Michigan a year later for a position at the Rockefeller Institute for Medical Research (RIMR). He drew on his experiences with his mentors at both institutions when he collaborated with Sinclair Lewis on the best-selling novel Arrowsmith. (See “Paul de Kruif and Microbe Hunters,” AAI Newsletter January/February 2019, for more information.)
At RIMR, de Kruif shared a laboratory with André Gratia, a Belgian microbiologist who came to the institute in 1920 to study bacteriophages. Gratia soon published papers on his discovery of a bacteriophage capable of infecting staphylococcus and E. coli. Gratia returned to Belgium in 1921 but had left an indelible mark on de Kruif. Gratia’s research was mirrored by that of the protagonist Martin Arrowsmith—both were pioneers in phage research and both discovered phages that would lyse staphylococcus.
Bacteriophage research would continue at RIMR and get a boost with the arrival of Jacque J. Bronfenbrenner (AAI 1920, president 1942–46) in 1923. Bronfenbrenner began a decades-long study of bacteriophages to explain their physical properties and understand and control their lysis. (Five years later, Bronfenbrenner accepted an appointment as chair of the Department of Bacteriology and Immunology at the Washington University School of Medicine in St. Louis and continued his phage research.)
1920s and AAI
Already widely investigated in Europe by the mid-1920s, bacteriophage research was sprouting up in laboratories beyond Ann Arbor and New York City. A survey of articles published in The Journal of Immunology (The JI) in the 1920s reveals phage research programs at Loyola University School of Medicine (Chicago), Baylor University, Yale University School of Medicine, and Stanford University. Compared to similar journals, such as the Journal of Experimental Medicine, The JI seems to have taken a cautious approach to publishing bacteriophage research, with a mere eight papers published during the decade. Likewise, it was not a topic featured prominently at the American Association of Immunologists (AAI) annual meetings; only two speakers on the subject presented their research: Emil Weiss (AAI 1928), “The Bacteriophage Anti-bacteriophage Reaction,” in 1927; and D. M. Cowie and Henry G. Poncher, “Observations on the Intestinal Bacteriophage in the Specific Infectious Diseases,” in 1928.
1930s
 Ad for bacteriophages
Ad for bacteriophages
NLMThe pace of phage research and phage therapy trials continued to accelerate well into the 1930s, but signs of problems with bacteriophage therapies were becoming more evident. Although bacteriophage therapy was “being widely used for many types of bacterial infection,” at the time, there were neither clear guidelines for clinical trials—the familiar control groups and double-blind studies were decades in the future—nor for the standardization of materials and methods. Considering the fact that scientists continued to debate whether bacteriophages were enzymes or viruses, it is understandable that the clinical studies were unable to generate accurate data on dosage, safety, and efficacy.
D’Hérelle emphasized that the crucial step in successful bacteriophagy was matching phage strain to the specific bacterial infection. This process, however, was both time consuming and labor intensive for individual clinical cases and exacerbated by the paucity of readily available phage strains. In an attempt to remedy part of this problem, pharmaceutical companies, including Eli Lilly & Co., E. R. Squibb & Sons, and Swan-Myers (a division of Abbott Laboratories), were “manufacturing bacteriophage and offering it to the medical profession.” A Journal of the American Medical Association (JAMA) review of the Lily, Squibb, and Swan-Myers phage preparations demonstrated the lack of standards—including the amount of preservatives or lack thereof, virulence, and mixture of different phage strains—and marked a further move away from d’Hérelle’s ideal bacteriophagy.
AMA Phage Report
Criticism of the purported successes of bacteriophagy increased in the early 1930s with titles such as “Limitations of Bacteriophage Therapy” appearing in journals. At this time, the American Medical Association (AMA) Council of Pharmacy and Chemistry, founded in 1905 to advocate for clinical experimentation and evaluate the “chemical identity and efficacy of drugs in humans,” began a review of bacteriophagy in scholarly literature. The first report was published in 1934, authored by two Yale University professors: immunologist and bacteriologist Stanhope Bayne-Jones (AAI 1917, president 1930–31) and infectious disease specialist Monroe Eaton (AAI 1937).
The report, “Bacteriophage Therapy: Review of the Principles and Results of the Use of Bacteriophage in the Treatment of Infections,” was published across three issues of JAMA in December 1934. In the report, the demonstrable ability of bacteriophage to lyse bacteria in vitro was recognized, but those results did not carry over into in vivo studies.
The authors reached the conclusions that “lytic action in the body is inhibited or greatly impeded by blood and other body fluids”; that the “therapeutic action” of the components mixed with the phage before injection needs additional study; that the literature “reveals that the evidence for the therapeutic value of lytic filtrates is for the most part contradictory”; and that “there is no evidence that lysis or killing of bacteria by bacteriophage occurs in vivo.”
Of particular interest is an additional conclusion reached by the authors: to accept that the “facts appear to indicate” bacteriophage is “inanimate, possibly an enzyme,” though they do leave the door open that it could be a virus. Bordet publicly tried to keep that door closed, stating during the prestigious Croonian Lecture in 1930 that the “invisible virus of d’Hérelle does not exist.” It is the bacteria themselves, subjected to the lysis, which reproduce the lytic principle. Bacteriophagy is accordingly a case of autolysis.” The Bordet theory about the nature of the bacteriophage remained dominant in the American scientific community.
The conclusions of the report, however, did not stop bacteriophage research and publication of results—better studies might be more successful. Indeed, phage research continued to spread, with new adherents like F. Macfarlane Burnet (AAI 1961), a young Australian researcher in England who would decades later win the Nobel Prize in Physiology or Medicine for discovering “acquired immunological tolerance.” While his phage research did not spawn breakthroughs in therapy, it did give Burnet insight into specificity, mutation, and resistance.
1930s and AAI
In the 1930s, The JI continued its conservative publication of articles related to bacteriophage research with only seven papers. One of these, however, directly challenged some of the conclusions of the AMA report. In their 1935 article “The Adaptation of a Staphylococcus Bacteriophage to an Artificially Produced Anti-Bacteriophagic Serum,” d’Hérelle and Morris L. Rakieten, who conducted bacteriophage research together at Yale University, disputed the claim that in vitro bacteriophagy was uniformly diminished by human serum and showed instead that some strains of bacteriophage were able to maintain lysis successfully in the presence of serum.
The AAI annual meetings at this time had a dearth of bacteriophage research with only two talks on the topic: Frances C. Frisbee and Ward J. MacNeal, “Therapeutic Application of Bacteriophage in Staphylococcus Bacteremia,” in 1932; and Philip Levine (AAI 1925) and Arthur W. Frisch (AAI 1938), “The Specificity of Multiplication of Bacteriophage,” in 1935.
The Decline of Phage Therapy
The issues of bacteriophagy outlined in the Bayne-Jones and Eaton JAMA report were clearly not insurmountable to the dedicated phage researcher, despite failure to demonstrate a successful therapy. What eventually moved the field away from phage research was the advent, expansion, and demonstrable success of sulfa drugs in the 1930s. Prontosil, patented in 1932, was cheaper and easier to produce and was effective against a wider variety of bacterial infections than bacteriophage therapy. Its success spawned a rush to put new sulfa drugs (and other antimicrobial chemotherapies) on the market.
In 1939, with Europe once again engulfed in a world war, non-war research ground to a halt. The United States would enter the war two years later, and scientific research likewise was quickly refocused to the war effort.
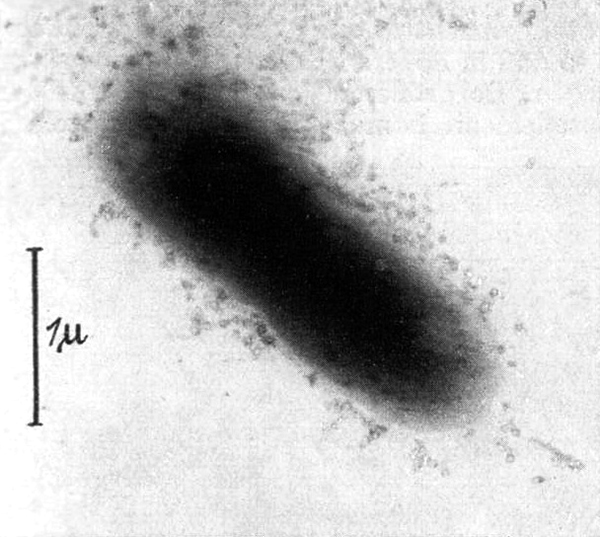 First phage electron micrograph
First phage electron micrograph
NaturwissenschaftenIn pre-war Germany, the electron microscope was developed and, before the war broke out, achieved sufficient magnification to capture the first images of viruses. When a bacteriophage sample was placed in the microscope in 1939, the picture that developed vindicated d’Hérelle—the bacteriophage was a virus. The image was published in a German scientific journal the following year. Due to the war, however, it would be a few years more before the debate was put to rest.
Bacteriophage therapy research did not end in the 1930s. It continued into the 1940s in the United States and Europe, only to finally be shelved in the archive following the discovery and development of antibiotics. D’Hérelle did continue his research in Ukraine, where, after the war, the Soviet Union had a national program dedicated to phage therapy.
Experience with bacteriophages altered the career trajectories of some researchers, including a young Alfred Hershey (AAI 1942) under the mentorship of Bronfenbrenner at Washington University. The lessons learned from studying the bacteriophage helped usher in a new field of biology following the war: molecular biology.
The JI and talks at the annual meetings told a different story for AAI. Evidence points to a conservative approach to bacteriophage research. Whether reflecting the fact that bacteriophages themselves were still not fully understood or that fundamentals of the immunological response to bacterial infections were still in dispute, it seems a cautious approach in the literature and at meetings proved a successful tack for the association and the field.
References
- American Association of Immunologists. Program of the Fourteenth Annual Meeting of the American Association of Immunologists, 1927. AAI Archive, Rockville, MD.
- American Association of Immunologists. Program of the Fifteenth Annual Meeting of the American Association of Immunologists, 1928. AAI Archive, Rockville, MD.
- American Association of Immunologists. Program of the Nineteenth Annual Meeting of the American Association of Immunologists, 1932. AAI Archive, Rockville, MD.
- American Association of Immunologists. Program of the Twenty-Second Annual Meeting of the American Association of Immunologists, 1935. AAI Archive, Rockville, MD.
- Bordet, Jules. “Croonian Lecture: The Theories of the Bacteriophage.” Proceedings of the Royal Society of London B 107, no. 752.
- Charnock, Donald A. “Phenomenon of Bacteriophagy,” American Journal of Surgery 19.
- Davis, Daniel M. The Beautiful Cure: Harnessing Your Body’s Natural Defenses Chicago: University of Chicago Press, 2018.
- D’Herelle, Felix. “Sur un microbe invisible antagoniste des bacilles dysentériques.” Comptes rendus de l’Académie des Sciences 165.
- D’Herelle, Felix. The Bacteriophage and Its Behavior. Translated by George H. Smith. Baltimore: Williams and Wilkins, 1926.
- D’Herelle, Felix and Morris L. Rakieten, “The Adaptation of a Staphlococcus Bacteriophage to an Artificially Produced Anti-Bacteriophagic Serum.” The Journal of Immunology 28, no. 6: 413–23.
- Eaton, Monroe D. and Stanhope Bayne-Jones. “Bacteriophage Therapy: Review of the Principles and Results of the Use of Bacteriophage in the Treatment of Infections.” Journal of the American Medical Association 103, no. 23: 1769–76.
- Eaton, Monroe D. and Stanhope Bayne-Jones. “Bacteriophage Therapy: Review of the Principles and Results of the Use of Bacteriophage in the Treatment of Infections.” Journal of the American Medical Association 103, no. 24: 1847–53.
- Eaton, Monroe D. and Stanhope Bayne-Jones. “Bacteriophage Therapy: Review of the Principles and Results of the Use of Bacteriophage in the Treatment of Infections.” Journal of the American Medical Association 103, no. 25: 1934–9.
- Fildes, Paul. “Frederick William Twort, 1877–1950.” Obituary Notices of Fellows of the Royal Society 7.
- Gratia, Jean-Pierre. “André Gratia: A Forerunner in Microbial and Viral Genetics.” Genetics 156, no. 2.
- Ho, Karen. “Bacteriophage Therapy for Bacterial Infections: Rekindling a Memory from the Pre-Antibiotics Era.” Perspective in Biology and Medicine 44, no. 1.
- “Limitations of Bacteriophage Therapy.” Journal of the American Medical Association 96, no. 9.
- Lingeman, Richard. Sinclair Lewis: Rebel from Main Street. New York: Random House, 2002.
- Sankaran, Neerajal. “Mutant Bacteriophages, Frank Macfarlane Burnet, and the Changing Nature of ‘Genespeak’ in the 1930s.” Journal of the History of Biology 43, no. 3: 571–99
- Straub, Margaret E. and Margaret Applebaum. “Studies on Commercial Bacteriophage Products.” Journal of the American Medical Association 100, no. 2.
- Summers, William C. “On the Origins of the Science in Arrowsmith: Paul de Kruif, Felix d’Herelle, and Phage.” Journal of the History of Medicine 46.
- Summers, William C. “The Strange History of Phage Therapy.” Bacteriophage 2, no. 2.
- Twort, Frederick W. “An Investigation on the Nature of Ultra-Microscopic Viruses.” Lancet 18, no. 4814.